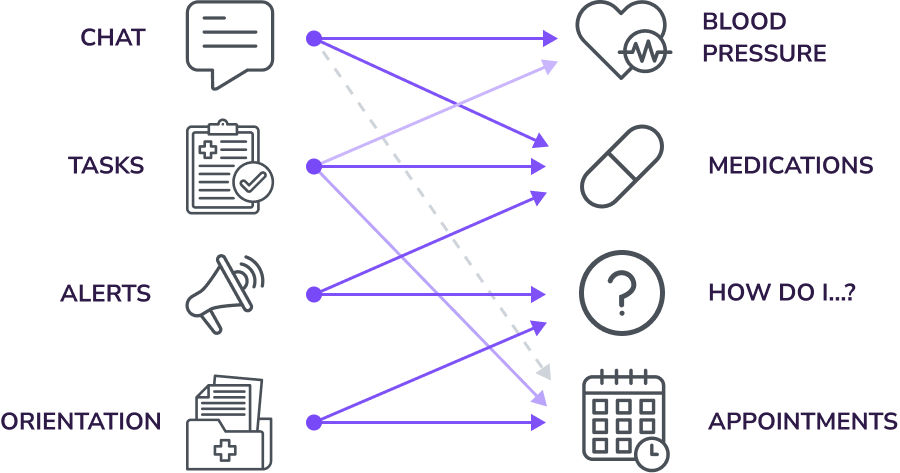
Defining Channels by Indicator Context
Based on each indicator’s type, relevance, and frequency, different patient contact channels were defined for each monitoring context. This ensured that health data was exchanged through the most appropriate channel, giving nurses and the system the right conditions to act on what patients reported.